
What's Next for AI in Healthcare? A Practical Analysis
- Riya ThambirajArtificial IntelligenceLast updated on

AI in healthcare delivers near-term ROI in administrative workflows -- clinical documentation automation (60-80% reduction in physician documentation time), AI-assisted billing and coding (3-5% revenue recovery from denial reduction), and prior authorization automation (40-60% processing time reduction). Diagnostic AI including imaging analysis and predictive risk scoring is advancing but requires longer regulatory validation timelines. Healthcare organizations should start with administrative AI before clinical AI because data quality requirements are lower and the regulatory burden is manageable.
The global healthcare IT market is projected to grow from USD 760.2 billion in 2024 to USD 1,834.3 billion by 2030. That growth is not speculative. It tracks the adoption of AI across clinical documentation, diagnostics, operations, and drug discovery.
Custom healthcare software development services are reshaping how care is delivered and how healthcare organizations run. The gains are real, but they are distributed unevenly. Some AI applications in healthcare pay back in months. Others require years of regulatory validation. Knowing the difference is what separates productive investment from expensive pilots.
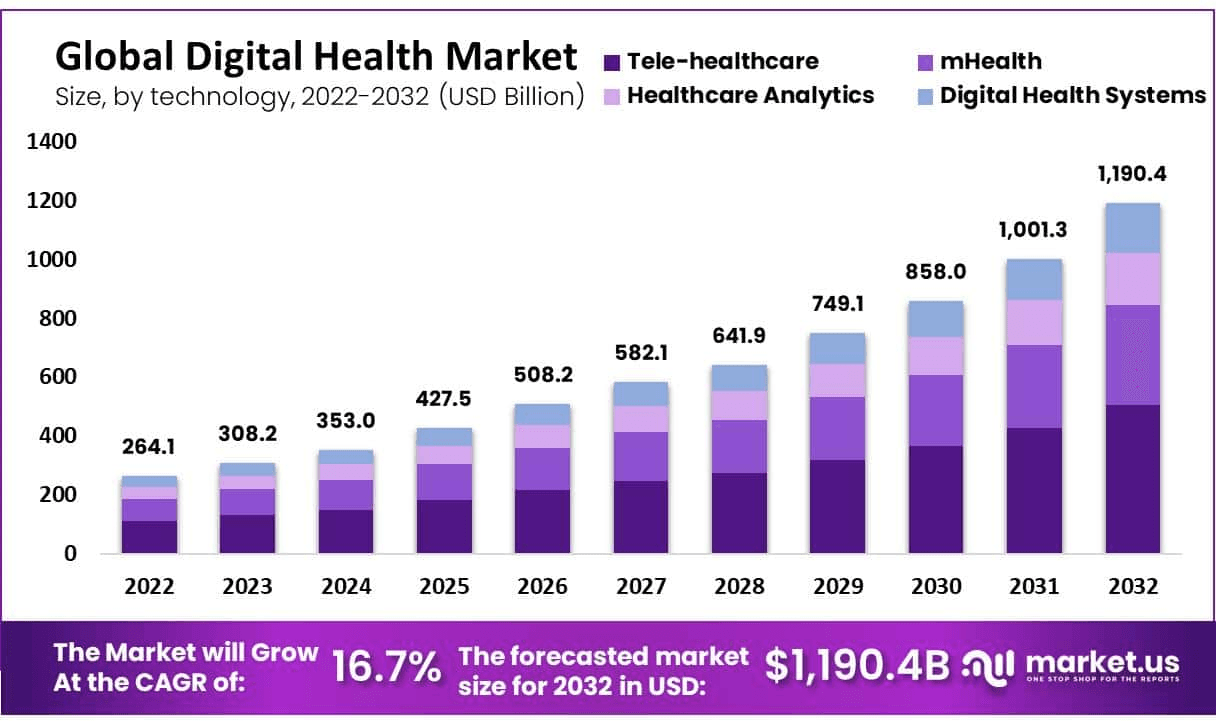
Source: https://media.market.us/digital-health-statistics/
AI in healthcare: where the ROI is now
At the core of healthcare software is one practical goal: improving care while reducing the cost of delivering it. AI addresses both, but the path differs by application.
AI-driven Electronic Health Records (EHRs). AI enhances EHRs by automating data analysis, identifying patterns in patient history, and, most practically, handling clinical documentation. Ambient documentation tools convert spoken notes to structured EHR entries, cutting documentation time by 60-80% per physician and reducing errors from manual transcription.
The technical integration standard for clinical AI is FHIR R4 (Fast Healthcare Interoperability Resources Release 4), which defines the API and data model that modern EHRs expose. CDS Hooks is the HL7 standard for embedding real-time AI alerts into EHR workflows -- a CDS Hook fires when a clinician opens a patient record or places an order, and the AI service responds with cards (alert messages, recommendations, order suggestions) that display inline in the EHR without requiring the clinician to navigate to a separate application. This is the architecture behind drug-drug interaction alerts, sepsis early warning scores, and medication dose recommendations in EHRs like Epic and Cerner.
For clinical NLP, BioBERT (pre-trained on PubMed and clinical notes) and Med7 (a spaCy model for clinical named entity recognition across 7 entity types: drug, dosage, frequency, duration, form, route, strength) extract structured data from free-text clinical notes at scale. Sepsis prediction models built on top of FHIR data combine qSOFA criteria (respiratory rate, altered mentation, systolic blood pressure) with trend data from lab results (lactate, creatinine, white cell count) to generate real-time risk scores. The same FHIR data layer enables diagnostic imaging AI: U-Net architectures for image segmentation identify organ boundaries and lesion regions in CT and MRI scans, with FDA 510(k) clearance required before clinical deployment in the US. The 510(k) pathway for AI/ML-based Software as a Medical Device (SaMD) applies to any software that makes or informs clinical diagnoses -- the FDA's 2021 AI/ML action plan and proposed regulatory framework for adaptive AI create a pathway, but clearance timelines of 12-24 months are typical for de novo clinical AI products.
AI-powered telemedicine. Telemedicine platforms integrated with AI add symptom checkers, automated follow-up scheduling, and predictive analytics. The telemedicine market, projected to exceed $130.5 billion by 2025, is pulling AI adoption with it.
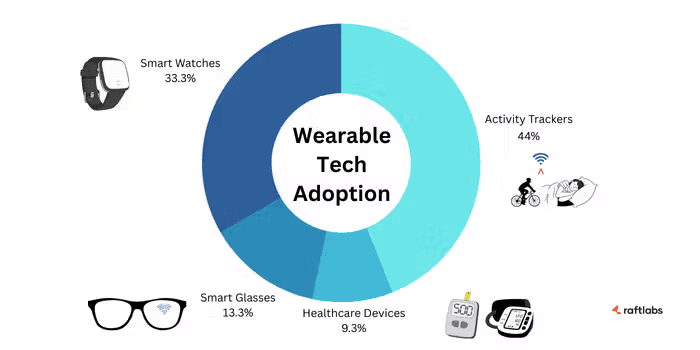
AI-enabled wearable health devices. Fitness trackers and smartwatches use AI to surface real-time health insights. These devices let patients monitor conditions and share actionable data with providers, enabling earlier intervention.
How AI streamlines healthcare operations
Healthcare AI is not just a clinical tool. It changes how healthcare organizations run the back office.
Hospital management systems (HMS). Appointment scheduling, patient record management, and billing are time-intensive and error-prone when handled manually. HMS platforms automate these tasks, freeing staff for direct patient care.
Prior authorization is where administrative AI delivers the clearest cost reduction in revenue cycle management. The CMS Interoperability and Prior Authorization Final Rule (effective 2027 for payers) mandates CRD (Coverage Requirements Discovery) and DTR (Documentation Templates and Rules) CDS Hooks, which means payers must expose their prior authorization rules as machine-readable APIs that EHRs can query in real-time. Healthcare organizations that build their PA workflow around these standards will have dramatically lower manual PA processing costs -- current industry estimates put PA processing at $31 per transaction manually, versus under $3 automated. HIPAA 5010 transaction sets govern the electronic claim submission layer: the 837P (professional) and 835 (remittance advice) formats are the standards for claim submission and payment posting. RCM automation that predicts claim denial before submission (gradient boosting on historical claim data, payer-specific denial patterns, and coding completeness checks) reduces initial denial rates by 15-25% in well-implemented systems. Appeal letter generation using LLMs trained on successful appeals further reduces write-offs on already-denied claims.
Appointment no-show prediction uses gradient boosting on patient demographics, appointment type, historical no-show pattern, scheduling lead time, and reminder response behavior to identify which appointments carry the highest cancellation risk. Models trained on 2-3 years of scheduling history typically achieve 70-75% accuracy on no-show prediction, enabling targeted double-booking of high-risk slots and personalized reminder escalation (SMS, phone call) for patients flagged as likely to miss. Bed capacity modeling using LSTM networks trained on historical length-of-stay data by DRG (Diagnosis Related Group), seasonality, and census patterns gives hospital operations teams a 24-72 hour forecast of bed availability that replaces the manual morning capacity huddle with a data-driven view.
Data-driven decisions. Machine learning and AI surface patterns in patient behavior, disease trends, and treatment outcomes that support faster, more accurate clinical and operational decisions.
Check out our Enterprise AI Development services for AI solutions for the healthcare industry.
How AI protects patient trust
In healthcare, data security is not optional. Healthcare software development addresses this through encrypted data storage, secure protocols, and compliance with HIPAA and GDPR. Every AI system touching patient data must be built with audit logging, role-based access controls, and business associate agreements with any vendor handling protected health information.
HIPAA Technical Safeguard requirements under §164.312 define the specific controls required: access controls (unique user identification, emergency access procedures, automatic logoff, encryption), audit controls (hardware, software, and procedural mechanisms to record and examine system activity), integrity controls (authentication of ePHI), and transmission security (encryption of ePHI in transit). De-identification is required for any data used in model training or shared with external parties: the Safe Harbor method removes all 18 specified identifiers (including name, dates of birth, geographic subdivisions smaller than a state, phone numbers, IP addresses, and device identifiers) before data can be used without individual authorization. The Expert Determination method requires statistical analysis confirming that re-identification risk is very small -- but in practice Safe Harbor is simpler to audit and easier to defend in an investigation.
Federated learning addresses the patient matching and multi-site model training challenge without data sharing. When a hospital system wants to train a sepsis prediction model on data from 12 sites, traditional approaches require centralizing patient data in a shared environment -- a significant privacy and compliance burden. Federated learning trains the model locally at each site, shares only model weight updates (not patient data) to a central aggregation server, and combines the updates into a global model. The result is a model trained on the full data distribution across all sites without any patient record leaving its originating facility. Patient matching across sites (when the same patient appears in multiple facility records) uses probabilistic matching combining MRN, demographic fields, and encounter dates rather than exact identifier matching, which fails at cross-organizational boundaries where MRNs differ. Deduplicate algorithms (Fellegi-Sunter probabilistic matching, or commercial solutions like Verato or MPI from Epic) are the standard infrastructure layer for master patient index management.
Also read: Conversational AI in healthcare -- key use cases and benefits.
Real-world AI deployments in healthcare
The results are not theoretical. Healthcare AI is already in production across diagnostics, documentation, and operations.
PDC Remote Patient Monitoring Software supports chronic care management with AI-assisted remote monitoring.
Google's AI imaging reduced breast cancer false negatives by 9.4% and false positives by 5.7%.
Canon Medical Systems' AiCE improves CT and MRI scan quality; Aidoc's AI identifies critical findings in medical images.
Nuance's Dragon Medical One converts spoken clinical notes to text, reducing documentation time and improving accuracy.
GE Healthcare's Command Center uses predictive analytics to optimize hospital staffing and equipment.
Google's DeepMind detects early signs of eye disease in diabetic patients, enabling timely intervention.
Emerging trends in healthcare AI
AI development services are accelerating across several high-impact areas.
AI analyzes genetic data and medical history to build personalized treatment plans, improving outcomes and reducing side effects.
Predictive analytics flags health risks earlier by detecting patterns in patient data. Cardiac events, sepsis, and readmission risk are the most validated applications.
Virtual health assistants and chatbots handle appointment scheduling, medication reminders, and FAQ responses around the clock.
AI-enhanced medical imaging analyzes X-rays, MRIs, and CT scans to detect abnormalities and prioritize urgent cases.
Drug discovery cycles are shortening as AI predicts drug efficacy and safety from genetic and clinical data.
Remote patient monitoring and telemedicine use AI to track vital signs and support proactive interventions.
Administrative automation (insurance claims, prior authorization, and scheduling) reduces cost without touching clinical decisions.
Surgical planning and robotics AI improves precision and outcomes in complex procedures.
Challenges in healthcare AI adoption
Innovation in healthcare AI is real. So are the barriers.
High initial investment. Custom solutions carry significant upfront costs. The long-term value justifies the expense, but organizations need realistic timelines to payback.
Integration complexity. Connecting new AI systems to legacy EHRs and clinical platforms requires careful architecture. Data pipelines need to be built for reliability and compliance, not just speed.
Ongoing maintenance. AI models drift. They require monitoring, retraining, and governance processes to stay accurate over time.
User adoption. Clinicians and administrators need training and change management support. AI tools deployed without adoption support see limited use.
Finding the right development partner. The right custom medical software development company understands both healthcare compliance and AI architecture. That combination is rare and worth selecting for carefully.
Despite these barriers, the direction is clear. Healthcare organizations that move now on administrative AI will recover revenue faster and build the data infrastructure that clinical AI depends on.
What to build next
Start with administrative AI. Prior authorization, medical billing, and scheduling have clear ROI, lower regulatory risk, and no clinical decision-making involved. Build the data infrastructure correctly from the start: encrypted, audited, and HIPAA-compliant by design, not by retrofit.
Invest in healthcare app development with the right architecture, and the path from administrative AI to clinical AI becomes much shorter.
If you want to build something practical in healthcare AI, schedule a free consultation. We will tell you honestly whether what we build fits your situation.
Frequently asked questions
- Machine learning will deepen its role in diagnostics, predictive analytics, and personalized treatment. The near-term priority is clinical documentation automation and EHR data analysis, where accuracy improvements are measurable and regulatory risk is lower. Longer term, ML will support earlier detection of conditions like cardiac events and sepsis by analyzing patterns in continuous monitoring data.
- Healthcare software will shift toward AI-augmented workflows rather than standalone tools. EHRs will gain ambient documentation (AI writes the note while the clinician speaks). Interoperability standards will improve data sharing across systems. And AI-assisted coding will become standard in billing, given the measurable revenue impact of reducing claim denials.
- Healthcare chatbots work well for a defined scope -- appointment scheduling, medication reminders, FAQ responses, and post-discharge follow-up. They do not replace clinical judgment. The key design requirement is a clean escalation path to a human when the query moves outside the defined scope. Scope creep is the most common failure mode.
- NLP converts unstructured clinical notes, discharge summaries, and physician dictations into structured data that downstream systems can use. This is where most healthcare AI value is unlocked -- not from new data collection, but from making existing documentation machine-readable. Ambient documentation products like Nuance Dragon Medical One are the most visible application.
- The fastest ROI comes from three areas -- AI-assisted medical billing (3-5% of revenue recovered from denial reduction), prior authorization automation (40-60% processing time reduction), and clinical documentation (60-80% reduction in physician documentation time). These are operational, not clinical, AI applications. The clinical applications (diagnostics, drug discovery) are real but have longer timelines and higher validation requirements.
- The highest-impact near-term trends are ambient clinical documentation, AI-assisted coding and billing, and predictive models for hospital capacity management. Longer term, multi-modal diagnostic AI (combining imaging, lab, and genomic data) and AI-accelerated drug discovery will have significant impact. The regulatory environment under FDA's AI/ML-based SaMD framework will shape clinical AI deployment timelines.
- AI in healthcare will have the most impact in three areas over the next five years -- administrative automation (documentation, billing, scheduling), diagnostic support (imaging analysis, predictive risk scoring), and drug discovery acceleration. Clinical AI will remain human-supervised. The economic case is clearest for administrative AI, which is why most healthcare organizations are starting there.
- AI can improve patient loyalty programs by identifying patients most likely to disengage, personalizing outreach based on health goals and visit history, and triggering timely follow-ups after care episodes. The data infrastructure is the same as what supports clinical AI -- a unified patient data layer that links behavioral signals to health outcomes.
From the blog

